DOCUMENTARY: Crisis And Hope [episode 1]
Owain Astles made this searing documentary about homelessness in Bristol and why we need to pay attention.

Illustration by Amber’s Illustrations
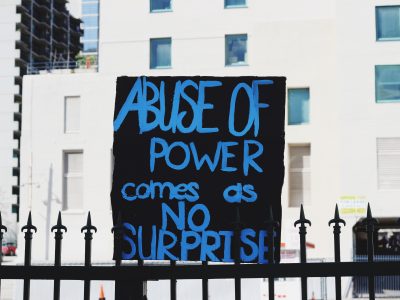
Neha describes the moment that she realised her race could affect how her patients saw her – and how racism affects medicine at large
On a dull October morning, four eager-to-impress Bristol University medical students sit in a GP clinic in the outskirts of Bristol. A white, male patient named James* limps into the office, nodding politely at the GP and the three white students before casting a cold glance in my direction. He exhales loudly. Check 1.
As the meeting progresses, James explains why he’s come into the clinic. He engages with the three white students seated next to me, whilst trying his hardest to turn his back towards my seat. Check 2.
‘Sir, since these students are shadowing me, I would like them to attempt to take a medical exam and check your blood pressure one at a time?’, the GP asks in a way that all doctors are accustomed too – respectfully gaining consent whilst knowing that they’re really the boss in the situation. ‘It’ll allow them to learn more about the clinical setting. Is that okay with you?’
He engages with the three white students seated next to me, whilst trying his hardest to turn his back towards my seat.
‘Yeah, yes of course. Why not?,’ James nods.
‘Great! Neha, why don’t you have a go first. And explain what you’re doing at each step of the exam -‘
‘Uhh – uhum, sorry excuse me’, James grunts, lines criss-crossing his suddenly pale forehead. Check 3.
‘No worries,’ says the GP. ‘Okay, Neha. Whenever you’re ready, have a go at taking James’ blood pressure.’
I nervously seat myself across James, who avoids my gaze as his own stays glued to the wooden floor. ‘Hello sir. I’d just like you to extend your arm out like this for me…sir?’, I ask hesitantly.
James, statue-like, continues to keep his gaze affixed on the floor. Check 4.
I extend a confused look to the GP, who returns a puzzled expression.
‘James, could you extend your arm straight out like this so she can put the cuff on. James… James, are you alright?’
Looking up, in what seems like the first time in forever, James sheepishly stares at the GP and mumbles, ‘I’m sorry, could someone else take the exam. I just… it’ll be easier for me, ya know?’ He looks around at the four white people around me, as if all of them can relate to what he’s feeling. Check, check, check.
And that was the moment I knew.
James sheepishly stares at the GP and mumbles, ‘I’m sorry, could someone else take the exam. I just… it’ll be easier for me, ya know?’
Everything sort of phased out until all I could hear was the quiet hum of the clinic. My three peers bowed their heads awkwardly as the GP, visibly flustered, changed the topic, desperate not to prolong this any further.
I was now a brown woman and nothing more.
I decided to enter the medical profession when I was 18. This decision was influenced by the doctors in my immediate family and the promise of financial security. However, as I made my way through the first few years of medicine, I was magnetically pulled into psychiatry. As someone who has suffered from depression and social anxiety, I knew how misunderstood mental health was across cultures and why this field needed people who could get down to their patients level to effectively diagnose and treat them.
But despite my faith in the inherent good of the medical system, when the aforementioned racially targeted incident occurred, I was instantly shaken. My belief in the medical profession, so solid before, had wavered. After a few months of silence, I began to share the details of the racially charged incident with others. Every single person asked the same thing: why didn’t you report this to the higher ups?
My belief in the medical profession, so solid before, had wavered.
I answered this the same way any other ethnic minority doctor or medical student would have – following any incident where we are racially targeted, we try to recognise the place of pain in the patient. We shrug off their comments and continue to uplift the patient’s interests above our own mental sanity. We would rather suffer indignity than draw attention to ourselves. And quite frankly, there has never been a strong culture of administrative support to shield doctors from racist patients. Just look at the incident I was involved in – there were four witnesses and one of them was my superior. No one did or said anything. It was simply brushed off.
A few years ago a study titled Racism in Medicine was published by a London health charity called Kings Fund. It examined how racism affected would-be doctors – before medical school, during medical school and after graduation or during the training years. The Kings Fund study showed, based on survey data, that white applicants with lower A-level grades were still more likely to be accepted than ethnic minority candidates with higher or equivalent grades. For women of colour who apply for a place in medicine a lack of guidance is combined with having to navigate a system which is inherently working against us.
For women of colour who apply for a place in medicine a lack of guidance is combined with having to navigate a system which is inherently working against us.
I spoke to many ethnic minority junior doctors for this article who worked in either the United Kingdom or the United States. To avoid racist comments from patients during medical rounds, a trend has emerged: ethnic minority medical students and doctors feel pressured to conform with the white environment. A few black junior doctors reported spending an exorbitant amount of time researching hairstyles which were considered appropriate for medical school and most resorted to wearing wigs rather donning their natural hair. Female Muslim students confessed to avoiding wearing a hijab in hospitals for fear of explicit and implicit racial bias.
I recall a clinical teaching session where medical students like myself were trained how to tackle verbal abuse and sexually inappropriate patients, but we weren’t once taught how to deal with racially abusive ones. Casual statements and questions like, ‘I would much rather see a white doctor,’ or, ‘but where are you really from?’ can make five or six years of rigorous medical training feel inadequate in a millisecond. Such remarks irrevocably impact the quality of care that healthcare workers can deliver – more so, it can have a detrimental effect on their mental health and wellbeing leading to decreased trust in the medical system and consequently, greater absenteeism.
Even after medical students graduate to become fully fledged doctors, racism still festers. The Kings Fund report found that despite there being a large number of capable ethnic minority doctors working in the NHS (22% of all NHS doctors are ethnic minorities), most of the sought-after medical fields were still dominated by white middle-class males.
Casual statements and questions like, ‘I would much rather see a white doctor,’ or, ‘but where are you really from?’ can make five or six years of rigorous medical training feel inadequate in a millisecond.
Everyone in the medical profession, especially white doctors, have a responsibility to pursue racial equality. We need to start addressing racism within the healthcare field the way we address racism everywhere else: by beginning to acknowledge its uncomfortable existence, pinpointing its identifiers and collaborating to end it in an institution which should not have a place for it. With Brexit looming, the NHS cannot afford to lose any more doctors, nurses and researchers. Wherever its workers come from, regardless of their country of training or place of birth, the NHS needs to be accepting.
One idea I support is to encourage UK medical universities and teaching hospitals to construct a mentor-mentee relationship for ethnic minority students and trainee doctors, providing support and guidance on how to handle doctor-patient interaction that’s peppered with racial bias.
In the University of Bristol Medical School alone there have been concerted efforts to increase representation for BME (Black and Minority Ethnic) medical students, through the creation of organizations like BME Medics, which aim to raise awareness about the lack of representation for BME medical students in academia and beyond and to foster a safe environment to discuss issues without fear of retribution. Other organisations like Melanin Medics, likewise, have dedicated themselves to supporting the community of African-Caribbean medical students and medical professionals in the UK and provide assistance to aspiring African-Caribbean medics.
We are progressing slowly. The General Medical Council and the British Medical Association are taking steps to discuss the effect of structural racism that affects medical school admissions and healthcare at large. There is a vital need to push the agenda of an egalitarian healthcare system globally and train doctors to respectfully challenge patients and doctors who hold discriminatory views.
As young doctors, our first primary task is to sign the Hippocratic Oath. We don’t judge patients and we provide a duty of care regardless of the colour of their skin or their religious affiliation. Because on our last breath, we’re all the same.
There is a vital need to push the agenda of an egalitarian healthcare system globally and train doctors to respectfully challenge patients and doctors who hold discriminatory views.
In my 21 years of life, I have encountered numerous people who have inadvertently passed comments which were steeped in stigma against ethnic minorities, otherwise known as microaggressions. From questions about how I spoke English so well for a Pakistani to being accused of belonging to the Taliban group by an elderly man. However, I never truly believed that microaggressions or even blatant racism could find its place within the healthcare system.
If I could go back in time, I’d tell my 18-year-old self many things to prepare her for the moment she realised the melanin in her skin was a marker of her identity. I’d tell her that this event was the first of many. I’d tell her that although she would be scarred in many places she didn’t know existed within her, she would also end up becoming stronger – yes, less vulnerable too, but much braver. I’d tell her that the journey of being a woman of colour is a lonely one. But, Neha, knowing you, you’ll use this opportunity to bring change for any young brown, black, Muslim girl or boy coming after you – because, well, you don’t want anyone else to ever feel the incomparable grief you felt because of one man.
Names marked with an asterisk (*) have been changed.
Follow Rife on Instagram, Twitter and Facebook.




Neha Maqsood is a 20-year-old, born-and-bred Pakistani currently pursuing a dual degree in Medicine and Global Health at Imperial College London and Bristol University. Alongside her academics, she is a part-time actress and radio show host. She starred in the 2018 film "Sisters in Arms," which is currently being shown at film festivals around the world, and hosted the award-winning radio show, "Will I ever be a Doctor?" under the Burst Radio Station. Most recently, she was listed as one of the 100 Most Influential BME (Black and Minority Ethnic) people in Bristol by Bristol 24/7 and Bristol Cable for her work in empowering ethnic minorities through leading a Women's March in Bristol and kick-starting a radio show calling out microaggressions against POCs on campus. Currently, she writes for multiple publications, including Epigram, Brown Girl Magazine, The Tempest and That's What She Said, about race, breaking through the Pakistani patriarchy and brown-feminism.